
The Similac® Liqui-Mix® System and Liquid Protein Fortifier can be used to customize calories and protein in an all-liquid solution.
The Similac® Liqui-Mix® System and Liquid Protein Fortifier can be used to customize calories and protein in an all-liquid solution.

All-liquid solution eliminates the need for most powder mixing
Easy to customize feedings, including 20, 24, 26, 27, and 28 cal/fl oz
Easy to customize protein levels with Liquid Protein Fortifier
Nutrient-enriched* preterm post-discharge formula shown to improve overall growth1
THE FIRST HUMAN MILK FORTIFIER WITH EXTENSIVELY HYDROLYZED PROTEIN†
Supported by 5 clinical studies, our human milk fortifier has been shown to deliver excellent outcomes.2-6


IMPROVED TOLERANCE3,4,6
IMPROVED BLOOD UREA NITROGEN (BUN) LEVELS2,4
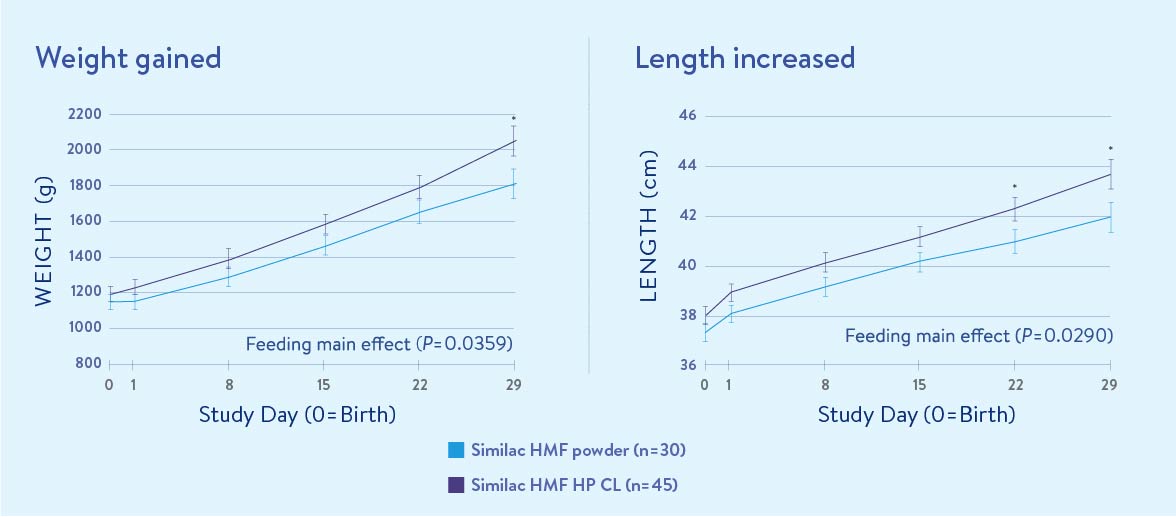
IMPROVED WEIGHT GAIN2-4,6,‡
FEWER ADVERSE EVENTS AND/OR LESS ACIDOSIS3-6
Packaged in single-use, ready-to-use packets for precise dosing and nutrient delivery
Liquid form reduces the risk for environmental contamination
Packets allow for aseptic handling when used as directed
Developed with a focus on safe handling for NICU use

Similac® offers the FIRST nonacidified human milk fortifier that has extensively hydrolyzed protein.
Similac HMF HP CL infants gained 0.5 lb more weight at study day 29, and both groups increased in weight and length over time
Similac HMF HP CL delivers 4.3g§ of protein (g/kg/day)
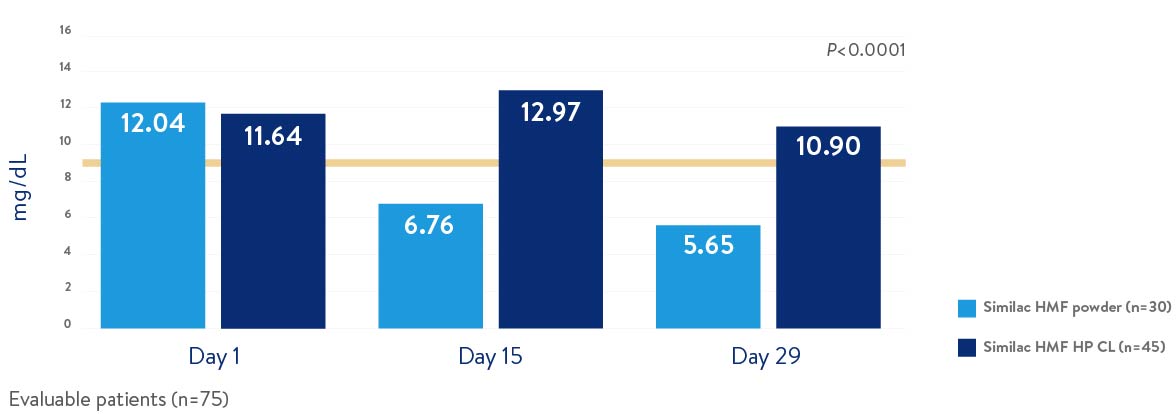
Evaluable patients (n = 75).¶
Hash marks indicate standard error.
ǁ Weight, g. Repeated Measures Analysis main effect, P = 0.036; post-hoc per timepoint analysis: SDAY 29, P = 0.024. Length, cm. Repeated Measures Analysis main effect, P = 0.029; post-hoc per timepoint analysis: SDAY 22, P = 0.006, SDAY 29, P = 0.037.
¶ These infants strictly adhered to study protocol and received ≥95% of their total intake from human milk with their assigned study fortifier.
Extensively hydrolyzed protein source to help promote easy digestion
Has OptiGRO® for brain and eye development
Low iron level provides flexibility to add iron as needed

Well tolerated
Only 1 in 66 (1.5%) NICU patients in the Similac HMF HP CL group discontinued due to feeding intolerance
No incidence of metabolic acidosis with infants fed Similac HMF HP CL or control
Improved protein status
Recent studies have identified BUN levels of >9 mg/dL as an indicator of protein sufficiency in preterm infants8-10
BUN levels remained above 9 mg/dL in preterm infants receiving Similac HMF HP CL
Mean BUN levels
EFFECTS OF AN ACIDIC pH ON HUMAN MILK
In vitro study of human milk acidified with citric acid to a pH of 4.511
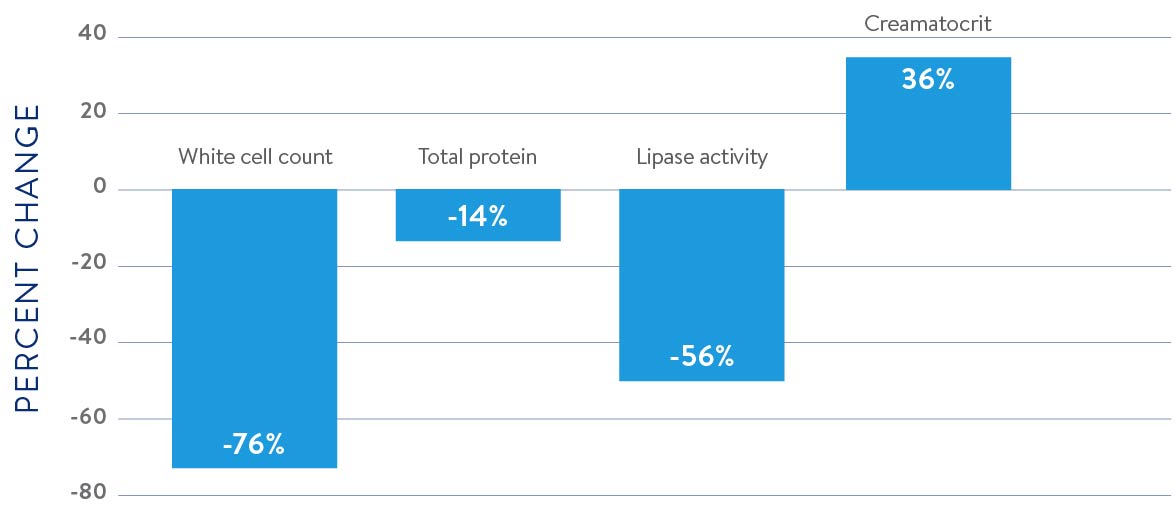
Similac HMF retains the pH of human milk to near neutral range, which should preserve the unique benefits of human milk.
* Increased protein, vitamins, and minerals compared to term infant formula.
† Launched in 2014. First nonacidified human milk fortifier that is hydrolyzed.
‡ In the Schanler study, weight gain was improved SDAY1-SDAY15.
§ Composition of human milk-based feedings at 120 kcal/kg and 24 Cal/fl oz.
References: 1. Carver JD, et al. Pediatrics. 2001;107(4):683-689. 2. Kim J, et al. J Pediatr Gastroenterol Nutr. 2015;61(6):665-671. 3. Kumar N, et al. Am J Perinatol. 2017;34(14):1411-1416. 4. Schanler RJ, et al. J Pediatr. 2018;202:31-37.e2. 5. Lainwala S, et al. J Neonatal Perinatal Med. 2017;10(4):393-401. 6. Clark B, et al. J Acad Nutr Diet. 2017;117(9 suppl 1):A11. 7. Kim JH, et al. J Pediatr Gastroenterol Nutr. 2015;61(6):605-671. 8. Arslanoglu S, et al. J Perinatol. 2006;26:614-621. 9. Alan S, et al. Early Hum Dev. 2013;89:1017-1023. 10. Ergenekon E, et al. Turk J Pediatr. 2013;55:365-370. 11. Erickson T, et al. J Perinatol. 2013;33:371-373.
Your sample eligibility has been revoked. You are no longer eligible to send samples to patients.
Would you like to submit this sample eligibility approval request to ?
Click “Yes” to confirm.
You are about to decline 's sample eligibility request.
Would you like to approve ’s sample eligibility request? This will be the only eligible user that you can approve to send samples while they are linked to your account.
Click “Yes” to confirm.
Would you like to revoke ’s sample eligibility?
Click “Yes” to confirm.
Would you like to submit this request to revoke your sample eligibility?
Click “Yes” to confirm.
Request has been declined.
Please be aware that the website you have requested to view is intended for Healthcare Professionals and may not be owned or maintained by Abbott. A new window will open in your browser once you select “yes”. You can return to this site by clicking the back arrow.
Do you wish to continue and exit this website?